读医学网

2012年呼吸机相关肺炎最新预防策略
发布时间:2014-05-20 09:24 类别:呼吸系统疾病 标签:diagnostic variability extreme criteria 来源:丁香园
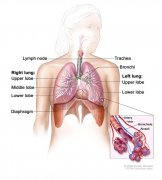
Ventilator-associated pneumonia (VAP) is a complication of mechanical ventilation and is defi ned as the occurrence of pneumonia in patients undergoing mechanical ventilation for at least 48 hours. Clinical suspicion of VAP arises when new infi ltrates are present on chest x-ray, and at least one of the following is present: Fever, leukocytosis, or purulent tracheo-bronchial secretions.
Th e incidence of VAP reported in the literature ranges from 15 to 20%. However, the real incidence of VAP is diffi cult to assess, given the extreme variability of the diagnostic criteria for pneumonia, which often rely on broncho scopic procedures. Th e specifi c mortality attributable to VAP is also debated. Th e reported VAPassociated mortality ranges from 20 to 70%. Patients with VAP are often critically ill, and survival may be aff ected both by underlying conditions and the new-onset VAP. A recent study demonstrated a relatively limited attributable intensive care unit (ICU)-mortality of VAP, about 1–1.5%, when adjusting for severity of co-existing diseases. In the last few years, various strategies have been investigated in order to reduce the incidence of VAP.
Reducing the duration of intubation, oral and endotracheal tube (ETT) care, positioning, and ETT modifi cations are aspects that may have a role in the prevention of VAP. Many of these strategies have been incorporated into ‘VAP bundles’, a set of treatments implemented simultaneously to reduce VAP incidence. Recent studies suggest that the use of bundle treatments can result in substantial reductions in rates of VAP.
In this chapter, we will present some novel VAP prevention strategies, explaining the possible mechanisms by which they may be clinically benefi cial in reducing the incidence of VAP. A summary of these novel strategies is given in Table 1.

- 猜你会喜欢....